
Translate this page into:
Intensive care unit mortality and length of stay among critically ill patients with sepsis treated with corticosteroids: A retrospective cohort study
*Corresponding author: Eric E. Chinaeke, PhD Department of Clinical Pharmacy and Outcomes Sciences, University of South Carolina College of Pharmacy, Columbia, SC, United States. ejikechinaeke@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Chinaeke EE, Yunusa I, Love BL, et al. Intensive care unit mortality and length of stay among critically ill patients with sepsis treated with corticosteroids: A retrospective cohort study. Am J Pharmacother Pharm Sci 2023; 5.
Abstract
Objective:
Sepsis is a major cause of morbidity and mortality in critically ill patients worldwide, and corticosteroids are commonly used to treat it. However, the evidence supporting the use of corticosteroids in sepsis patients admitted to the intensive care unit (ICU) is of low certainty, with conflicting results reported in previous studies. Thus, we aimed to investigate the potential association between corticosteroid treatment and various outcomes, including 30-day ICU mortality, ICU length of stay (LOS), mechanical ventilation use, new onset of infection, and hyperglycemia in patients diagnosed with sepsis and admitted to the ICU.
Materials and Methods:
We conducted a cohort study utilizing data from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database from 2008 to 2019. The study compared users of corticosteroids following admission to the ICU with non-users. Outcomes assessed included 30-day ICU mortality, ICU length of stay (LOS), mechanical ventilation use, new onset of infection, and hyperglycemia. Doubly robust, augmented inverse propensity weighted models were employed to control for confounders and determine the average treatment effect (ATE) of corticosteroids on study outcomes.
Results:
A total of 10,098 patients with a first diagnosis of sepsis were identified, of which 1,235 (12.2%) received corticosteroid treatment, and 8,863 (87.8%) did not. Corticosteroid use was associated with increased 30-day ICU mortality (ATE, 0.127; 95% CI, 0.083 to 0.171), ICU LOS (ATE, 1.773; 95% CI, 1.036 to 2.510), mechanical ventilation use (ATE, 0.181; 95% CI, 0.130 to 0.233), new onset of infection (ATE, 0.063; 95% CI, 0.032 to 0.094), and hyperglycemia (ATE, 0.024; 95% CI, 0.013 to 0.035) compared to non-use.
Conclusion:
The safety profile of corticosteroid therapy in sepsis patients admitted to the ICU remains a concern. Clinicians should carefully consider all available evidence and patient preferences when deciding to prescribe corticosteroids. Given the low certainty of evidence supporting the current treatment guidelines, further research is warranted to provide a more conclusive understanding of the risks and benefits associated with corticosteroid use in this patient population.
Keywords
septic shock
corticosteroids
mortality
length of stay
critical care
organ dysfunction scores

INTRODUCTION
Sepsis is a major contributor to mortality rates in the United States, and the standard pharmacologic treatment involves antibiotics, fluids, and vasopressors as needed.[1,2] Despite tremendous progress in understanding its underlying mechanisms of sepsis, drugs targeting specific cytokine cascade pathways have not conclusively improved patient survival.[3,4] As a result, corticosteroids have been used as adjuvant therapy for sepsis for decades.[5] However, their safety and effectiveness in patients admitted to the intensive care units (ICUs) remain uncertain.[6,7]
The previous randomized clinical trials (RCTs) have linked high-dose corticosteroid use with increased morbidity and mortality.[8,9] However, the results of studies examining the effects of lower-dose corticosteroids on sepsis mortality are mixed.[3,10] Systematic reviews of several observational studies and RCTs have not provided compelling evidence for or against the use of corticosteroids in patients with sepsis or septic shock.[11] Some studies suggest that the use of corticosteroids is associated with reduced mortality and ICU length of stay (LOS).[6] others did not.[7,12]
Lu et al. used a publicly available clinical database to investigate corticosteroid use in patients with sepsis admitted to the ICU. They found no association between corticosteroid use and a decreased risk of infection, ICU LOS, or mortality.[7] Conversely, Britt et al. found that corticosteroid use was associated with an increased risk of infection, ICU LOS, prolonged ventilator LOS, and mortality.[12] Current clinical practice guidelines recommend using corticosteroids in patients with septic shock only after adequate fluid resuscitation and vasopressor treatment have failed to restore hemodynamic stability. However, the guidelines classified the recommendation as weak due to the low quality of available evidence.[13]
Given the lack of consensus on the usefulness of corticosteroids for reducing sepsis mortality, clinical practices vary widely. Therefore, real-world studies are needed to add to the totality of evidence regarding the outcomes of corticosteroid use in patients with sepsis. As a result, we conducted a retrospective cohort study of patients with sepsis admitted to the ICU to evaluate the treatment effect of corticosteroids on 30-day ICU mortality and ICU LOS.
MATERIALS AND METHODS
Data sources
This study utilized the Medical Information Mart for Intensive Care-IV version 0.4 (MIMIC-IV v 0.4) database. Data were retrospectively collected from the hospital wide Electronic Health Record and an ICU specific clinical information system of the BIDMC between 2008 and 2019.[14] MIMIC-IV v 0.4 is an upgraded iteration of the MIMIC-III database that features contemporary data, more years of data collection, and additional variables to make it more user-friendly for healthcare research purposes. The STrengthening the Reporting of OBservational Studies in Epidemiology statement was adhered to in reporting the findings of this study.[15]
The study retrospectively analyzed a cohort of adult patients who were 18 years or older and were admitted to any of the ICUs (including coronary care unit, cardiac surgery recovery unit, surgical ICU, trauma/surgical ICU, medical ICU, and medical/surgical intensive unit) at BIDMC between 2008 and 2019.[14] MIMIC-IV v0.4 database is a large, de-identified, comprehensive critical care database of patients admitted to BIDMC ICU.[14] MIMIC-IV is rich in patient’s bedside information such as vital signs, laboratory data, prescriptions and medical charts, procedural and the International Classification of Diseases, Ninth and Tenth Revision (ICD-9-CM and ICD-10-CM) codes.[14] The Laboratory for Computational Physiology at Massachusetts Institute of Technology utilized structured data cleansing and date shifting to de-identified data in accordance with the Health Insurance Portability and Accountability Act standards.[14]
Sepsis patients selection and definition
This study is designed as a diagnosis-based cohort entry restricted to admission into the ICU as shown in [Figure 1]. We defined patients with sepsis using the modified Angus abstraction criteria and relevant ICD-9-CM and ICD-10-CM codes. The abstraction process and programming was performed as described in Horng et al. and Iwashyna et al.[16,17] and as programmed in the MIMIC Laboratory for Computational Physiology retrieved from mimic GitHub, Inc website (https://github.com/MIT-LCP/mimiccode/blob/master/concepts/sepsis/angus.sql). Specifically, we utilized a set of ICD-9-CM and ICD-10-CM codes and procedure codes for infection, acute organ dysfunction, and mechanical ventilation to retrospectively identify patients with severe sepsis. The Angus abstraction was then modified by including additional new ICD-9-CM and ICD-10-CM codes for sepsis, severe sepsis, septic shock and codes indicative of viral meningitis, cholangitis, and orbital cellulitis.[16,17] A total of 13,425 patients with their first ICU admission for first sepsis diagnosis between 2008 and 2019 or latest data available were identified. Patients with zero (0) or missing sequential organ failure assessment (SOFA) score were excluded from the study. Patients younger than 18 years of age and with missing data or without documented laboratory tests and vital signs taken within the first 24 h of ICU admission were excluded from the study. For patients with multiple vital signs or laboratory tests records in the first 24 h, average record was considered.
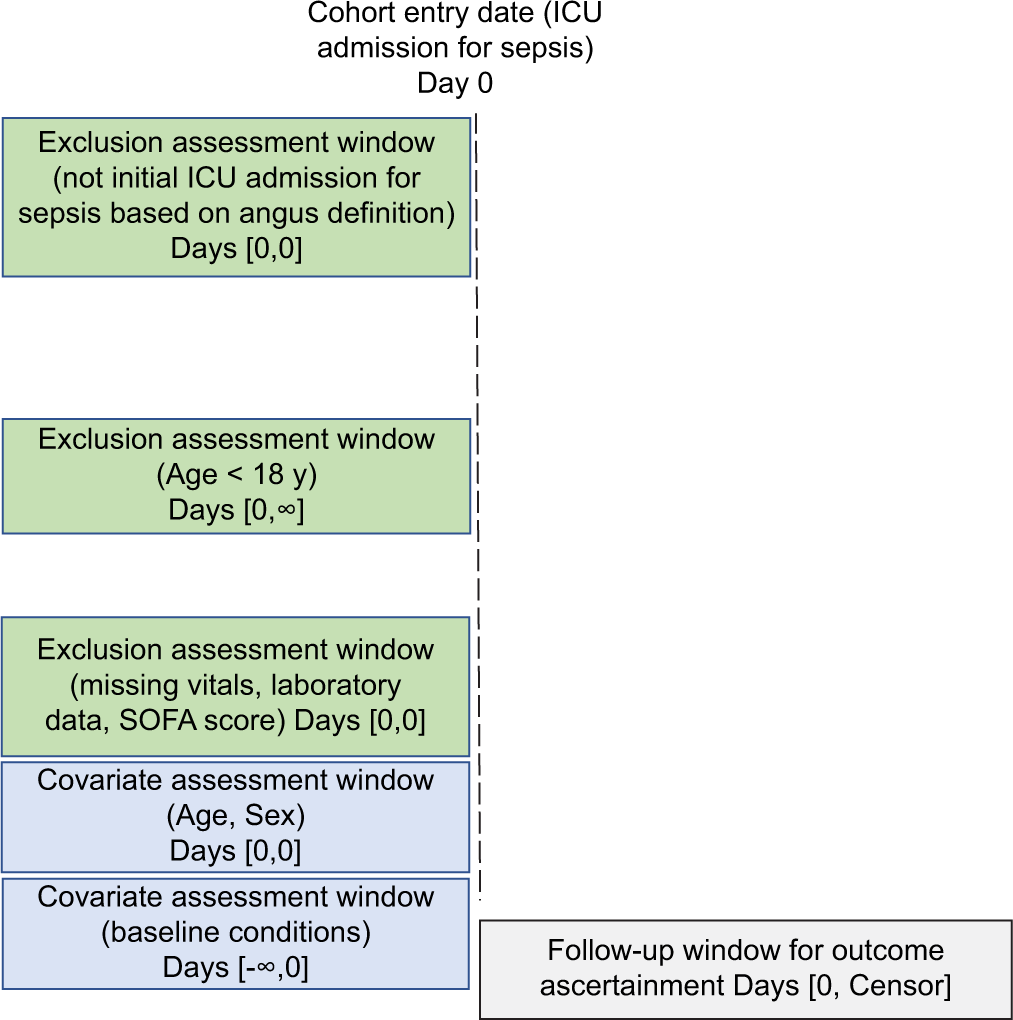
- Sepsis diagnosis-based cohort entry restricted to ICU admitted patients where the cohort entry date is selected after application of exclusion criteria. ICU: Intensive care unit; SOFA score: The Sequential Organ Failure Assessment.
Steroids exposure
We used the MIMIC-IV v 0.4 prescriptions drug file and pharmacy file to identify steroid use based on generic name, brand names and NDC codes. To assess the effects of steroid use on 30-day ICU mortality, ICU LOS, mechanical ventilation, new onset of infection, and hyperglycemia, patients were categorized into “steroid users” and “non-users.” The index date was established as either the first recorded date of steroid prescription or the date of ICU admission for patients who did not receive a prescription for steroids. Patients who had a record of prescription for any of the listed systemic corticosteroids (including hydrocortisone, dexamethasone, and methylprednisolone) following a diagnosis of sepsis were classified as steroid users, while non-users were defined as patients without prescription records for any of these types of corticosteroids.
Clinical outcome
The study’s primary outcomes were 30-day ICU mortality and ICU LOS, while its secondary outcomes included mechanical ventilation, new onset of infection, and hyperglycemia. To determine mortality within 30 days of ICU admission, the “INTIME” (ICU admission date and time), “OUTTIME” (ICU discharge date and time), date of admission “ADMITTIME,” and date of discharge “DISCHTIME” variables from both the admission and ICU stay files of the Mimic IV v0.4 database were utilized.[14] Patients who had a record of death within 30 days of ICU admission were classified as “Yes,” while those who did not have a record of death within 30 days of ICU admission were classified as “No.”[14] The “ICUSTAYS” file was used to measure ICU LOS in fractional days, which was defined as “the LOS for the patient for the given ICU stay.[14]
Mechanical ventilation outcome following treatment with steroids was determined using relevant procedural codes and categorized into mechanical ventilation “Yes” or “No.” New onset of infection was determined based on positive fungal and or bacteria blood culture after the index dates. Urine and sputum culture data were not available to be considered. Patients with record of positive blood culture for any of the infections were categorized as “Yes” while patients with negative blood culture for any of the infection were categorized as “No.”[14] Diagnosis of hyperglycemia was determined based on mean blood glucose levels ≥180 mg/dL after the index date consistent with the surviving sepsis campaign’s definition of hyperglycemia.[13] Patients with mean blood glucose level ≥180 mg/dL were categorized as “Yes” while patients with mean blood glucose level <180 mg/dL were categorized as “No.”
To analyze the secondary outcomes, patients who had a mean blood glucose level of 180 mg/dL or higher, received mechanical ventilation, or had positive blood cultures for bacteremia and/or fungemia before the index date were excluded from the analysis.
Covariates
This study controlled for various covariates such as demographic characteristics: Example age gender, race category, and health insurance. Clinical characteristics such as vital signs, laboratory tests, body mass index (BMI), Elixhauser comorbidity index (ECI),[18] statin use, ICU subtypes, and the SOFA score were included. Severe sepsis and septic shock diagnostic codes were excluded in the calculation of ECI. BMI (in kg/m2) was calculated by accessing records of patient’s height taken on the given hospitalization period and the patients weight taken within the first 24 h of corresponding patient’s first ICU stay. SOFA score was calculated using the algorithm retrieved from the GitHub, Inc website (https://github.com/MITLCP/mimic-code/blob/master/concepts/severityscores/sofa.sql) based on the data obtained during the first 24 h of patient’s first ICU stay. Laboratory tests (Mmol/L) included were hemoglobin, albumin, white blood cell and bicarbonate. Heart rate (in beats per minutes) was the vital sign included. Laboratory test parameters included in the SOFA score calculation was not included as a covariate in the multivariable modeling.
In addition, we controlled for statin use in the ICU given the evidence of its anti-inflammatory/pleiotropic effects in patients with sepsis in the ICU and the potential effects on the study outcomes.[19] ICU subtypes were categorized into medical ICU, coronary/cardiac (coronary and cardiac surgery ICU), trauma/surgical ICU (trauma and surgical ICU), and Medical/Surgical ICU.
Statistical analysis
We described patient’s baseline characteristics using frequencies and percentages for categorical variables. Mean with standard deviation and median with interquartile range were used to describe continuous variables such as the SOFA score, laboratory test results, and vital signs. In the multivariate analysis, we used a doubly robust estimation based on augmented inverse probability weighting (AIPW) to determine the average treatment effect (ATE) of steroids use. AIPW involves a simultaneous combination of propensity score modeling and outcomes modeling to generate potential outcome means (POM) for exposed/unexposed groups, and the ATE which is the difference between the POM for exposed group (steroid users) and POM for unexposed group (non-users).[20]
The concept of the AIPW estimation approach involves generation of a doubly robust ATE estimates which is unbiased even in the event of a mis-specification of one of the models.[20] The propensity score modeling component constitutes a generation of balancing score for different patient characteristics between exposed and unexposed groups through principles of weighting. Thus, weighting ensures that measured patient characteristics are balanced between steroid users and non-users as obtained in a RCT.[20] Balanced patient’s characteristics across users and non-users is required to establish a causal interpretation of the effect of steroids. Patient’s characteristics balance is assessed using standardized differences. Weighted standardized differences closer to zero (0) compared to the unweighted standardized differences is considered balanced across treatment and control group.[20] In other words, a standardized mean difference <0.1 means that the steroid users and non-steroid users groups are balanced in terms of observed covariates. For standardized mean difference >0.1, the groups are considered imbalance.[21]
In this study, we estimated the ATE of steroid use on 30-day ICU mortality, ICU LOS, mechanical ventilation, new onset of infection, and diagnosis of hyperglycemia. ATE represents a calculated difference between the POM of steroid users and non-users. ATE were considered significant at an alpha level <0.05.
Sensitivity analysis
Use of corticosteroids in this study was categorized as “Yes” for the presence of corticosteroids prescriptions-systemic methylprednisolone, dexamethasone, and hydrocortisone and “No” for no corticosteroid prescription without considerations for dosing and duration. We performed a sensitivity analysis considering dosing and duration of corticosteroid use. We categorized low dose-long duration (<400 mg corticosteroid equivalent for >3 days) and high dose-short duration (>400 mg corticosteroid equivalent for <3 days). Given that our feasibility study results a small sample size for high dose-short duration sub-group, we then compared low dose-long duration corticosteroid categories with category without corticosteroid prescription to generate ATEs.
Ethical Approval
The University of South Carolina’s institutional review board granted approval on May 7, 2021, for Project Pro00100865 and confirmed its exemption from the regulations governing research on human subjects.
RESULTS
We restricted patient population to adult patients with first sepsis diagnosis and the corresponding ICU admission as shown in [Figure 1]. In [Figure 2], we present the flow chart of the cohort selection process including application of various inclusion and exclusion criteria as well as the final analytical sample. From the MIMIC-IV v0.4 database, a total of 54,911 hospitalized patients diagnosed with sepsis based on modified angus abstraction between 2008 and 2019 were identified. We identified 13,425 adult patients with first diagnosis of sepsis and first ICU admission. After, applying exclusion and inclusion criteria, we identified in the final sample, 1,235 who were treated with steroids (steroid users) and 8,863 who were not treated with steroids (non-users).

- Flow chart on the cohort selection process.
[Table 1] provides an overview of the baseline characteristics of the individuals included in the study, categorized by their steroid prescription status. The table includes both unweighted and weighted standardized differences calculated using the AIPW method. The weighted standardized differences were below 0.10 and were smaller than the values obtained for unweighted standardized differences, indicating a balanced distribution of characteristics between steroid users and non-users.
| Characteristics | Steroid prescription | Standardized difference | ||||
|---|---|---|---|---|---|---|
| Steroid users (n=1,235) | Non-users (n=8,863) | |||||
| n | % | n | % | Unweighted | Weighted | |
| Demographic characteristics | ||||||
| Age group | ||||||
| 18–50 (Ref) | 278 | 22.51 | 1638 | 18.48 | ||
| 51–79 | 552 | 44.70 | 3166 | 35.72 | 0.1707 | −0.0016 |
| 80+ | 405 | 32.79 | 4059 | 45.80 | −0.2904 | −0.0432 |
| Gender | ||||||
| Female (Ref) | 606 | 49.07 | 4290 | 48.40 | ||
| Male | 629 | 50.93 | 4573 | 51.60 | −0.0215 | 0.0245 |
| Race | ||||||
| White (Ref) | 795 | 73.95 | 5758 | 77.29 | ||
| Black | 135 | 12.56 | 734 | 9.85 | 0.0688 | 0.0273 |
| Others | 145 | 13.49 | 958 | 12.86 | 0.0949 | 0.0247 |
| Insurance | ||||||
| Medicaid (Ref) | 95 | 7.69 | 700 | 7.90 | ||
| Medicare | 549 | 44.45 | 4373 | 49.34 | −0.1534 | −0.0268 |
| Others | 591 | 47.85 | 3790 | 42.76 | 0.0924 | 0.0096 |
| Clinical characteristics | ||||||
| Statin prescription | ||||||
| Non-users (Ref) | 1040 | 84.21 | 6878 | 77.60 | ||
| Users | 195 | 15.70 | 1985 | 22.40 | −0.0914 | −0.0929 |
| Modified Elixhauser comorbidity index | ||||||
| 0 (Ref) | 214 | 17.30 | 1603 | 18.09 | ||
| 1 | 589 | 47.70 | 4113 | 46.40 | 0.0057 | 0.0129 |
| 2+ | 432 | 35.00 | 3147 | 35.51 | −0.0914 | −0.0929 |
| Intensive care unit types | ||||||
| Surgical ICU (Ref) | 330 | 27.94 | 2457 | 28.99 | ||
| Cardio-coronary ICU | 127 | 10.75 | 1525 | 18.00 | −0.235 | −0.1213 |
| Medical ICU | 386 | 32.68 | 2586 | 30.52 | 0.0929 | 0.0101 |
| Medical/surgical intensive ICU | 338 | 28.62 | 1906 | 22.49 | 0.0008 | 0.0446 |
| Laboratory tests (Mmol/L): (Median[IQR]) | ||||||
| Albumin | 3.6 (1.9–5.0) | 3.1 (1.0–4.8) | −0.1218 | −0.019 | ||
| White blood cell | 11.1 (7.4–20.1) | 13.4 (8.4–21) | 0.1116 | −0.2446 | ||
| Hemoglobin | 11.7 (7.7–15.6) | 12.54 (6.2–18.7) | −0.3619 | −0.0093 | ||
| Bicarbonate | 25.0 (11.0–47.0) | 24.6 (7.0–40.0) | 0.0992 | 0.0648 | ||
| Vital signs | ||||||
| Heart rate (in beats per minutes) | 90 (77–106) | 101 (84–111) | 0.0090 | −0.0050 | ||
| Body mass index (kg/m2) | 24.2 (16–37.5) | 26.1 (15.1–37.2) | 0.0132 | −0.0137 | ||
| SOFA score, mean (SD) | 8.4 (4.01) | 7.9 (3.71) | 0.0281 | −0.0039 | ||
ICU: Intensive care unit, SOFA: The sequential organ failure assessment, IQR: Interquartile range, kg/m2: Kilogram/meter square, AIPW: Augmented inverse probability weighting, mmol/L: Millimoles/liter, Ref: Reference
[Table 2] shows crude estimates of steroid use on 30-day ICU mortality, ICU LOS, mechanical ventilation, new onset of infection, and incidence of hyperglycemia. A total of 1,732 patients died in the ICU within 30 days of admission of which 324 patients were treated with steroids. 30-day ICU mortality was significantly different between steroid users versus non-users (P < 0.0001). Average ICU LOS was higher among steroids users compared with non-users (7.08 vs. 5.20 days; P < 0.0001). Crude assessment shows that steroid users had higher average ICU LOS than non-users by 2.6 fractional days on average. A total of 3,166 patients were incident users of mechanical ventilation after index date.
| Steroids prescription | P-value | ||||
|---|---|---|---|---|---|
| Steroid users (n=1235) | Non-users (n=8863) | ||||
| n | % | n | % | ||
| Primary outcomes | |||||
| 30-day ICU mortality | |||||
| No | 893 | 72.31 | 7455 | 84.11 | <0.0001 |
| Yes | 324 | 27.69 | 1408 | 15.89 | |
| ICU length of stay (fractional days) | |||||
| n | 1235 | 8863 | <0.0001 | ||
| Mean | 7.08 | 5.2 | |||
| Std. Dev | 8.16 | 6.45 | |||
| Secondary outcomes | |||||
| Mechanical ventilation | |||||
| No | 720 | 58.3 | 6212 | 70.09 | <0.0001 |
| Yes | 515 | 41.7 | 2651 | 29.91 | |
| New onset of infection | |||||
| No | 761 | 61.6 | 6204 | 70 | <0.0001 |
| Yes | 474 | 38.4 | 2659 | 30 | |
| Hyperglycemia | |||||
| No | 74 | 6.1 | 1861 | 21 | <0.0001 |
| Yes | 1160 | 93.9 | 7001 | 79 | |
ICU: Intensive care unit, n: Number, Std. Dev: Standard deviation
Crude estimation shows that incident use of mechanical ventilation was significantly lower in steroids users versus non-users (P < 0.0001). A total of 8,161 patients experienced hyperglycemia following index date. Crude estimation shows that new diagnosis of hyperglycemia was significantly lower in steroids users versus non-users (P < 0.0001).
The result in [Table 3] shows the ATE of steroids on various primary and secondary outcomes after adjusting for confounders. Steroid use significantly increased average 30-day ICU mortality compared to non-use (ATE, 0.127; 95% confidence interval [CI], 0.083–0.171; P < 0.0001). Steroid use significantly increased average ICU LOS of patients with sepsis compared to non-use (ATE, 1.773; 95% CI, 1.036–2.510; P < 0.0001). Considering the secondary outcomes, steroid use significantly increased the incidence of mechanical ventilation use compared to non-users (ATE, 0.181; 95% CI, 0.130–0.233; P < 0.0001). Steroid use significantly increased new onset of infection compared to non-steroid use (ATE, 0.063; 95% CI, 0.032–0.094; P < 0.0001). Steroid use significantly increased the incidence of hyperglycemia compared to non-steroid use (ATE, 0.024; 95% CI, 0.013–0.035; p = 0.0004).
| Steroid users versus non-steroid users | |||||||||||||
| Primary outcomes | |||||||||||||
| 30-day ICU mortality | ICU length of stay | ||||||||||||
| Estimate | Wald 95% CL | P | Estimate | Wald 95% CL | P | ||||||||
| Parameter | |||||||||||||
| POM | Steroid Users | 0.256 | 0.214 | 0.298 | <0.0001 | 6.583 | 5.880 | 7.285 | <0.0001 | ||||
| POM | Non- users | 0.128 | 0.115 | 0.142 | <0.0001 | 4.810 | 4.572 | 5.048 | <0.0001 | ||||
| ATE | 0.127 | 0.083 | 0.171 | <0.0001 | 1.773 | 1.036 | 2.510 | <0.0001 | |||||
| Secondary outcomes | |||||||||||||
| Mechanical ventilation | New onset of infection | Hyperglycemia | |||||||||||
| Estimate | Wald 95% CL | P | Estimate | Wald 95% CL | P | Estimate | Wald 95% CL | P | |||||
| Parameter | |||||||||||||
| POM | Steroid users | 0.467 | 0.419 | 0.515 | <0.0001 | 0.107 | 0.077 | 0.137 | <0.0001 | 0.046 | 0.036 | 0.057 | <0.0001 |
| POM | Non- users | 0.286 | 0.267 | 0.304 | <0.0001 | 0.044 | 0.035 | 0.052 | <0.0001 | 0.022 | 0.018 | 0.025 | <0.0001 |
| ATE | 0.181 | 0.130 | 0.233 | <0.0001 | 0.063 | 0.032 | 0.094 | <0.0001 | 0.024 | 0.013 | 0.035 | 0.0004 | |
POM: Potential outcome means, ATE: Average treatment effect, CL: Confidence limit, P:P-value. Each model controlled for: Age group, race Category, insurance, SOFA score: The sequential organ failure assessment, laboratory tests and vital signs, MECI: Modified Elixhauser comorbidity index, ICU subtypes, statin use, BMI, and data year category. Statistically significant at alpha significance level ≤0.05
The sensitivity analysis revealed that there was no significant difference in the ATEs when comparing subgroups of individuals who received low-dose, long-duration corticosteroid treatment with those who did not receive any corticosteroid treatment [Supplementary table 1]. Specifically, the ATEs generated were similar in magnitude and direction to those obtained when corticosteroid prescription was dichotomized into “yes” or “no” categories.
DISCUSSION
Among patients admitted to the ICU and who were diagnosed with sepsis, we found that, the use of corticosteroids significantly increased average 30-day ICU mortality, average ICU LOS, incidence of mechanical ventilation use, new onset of infection and incidence of hyperglycemia. Our findings are consistent with previous studies that examined impact of corticosteroid on patients with sepsis or septic shock admitted in the ICU. Britt and colleagues conducted a case-control study of patients treated with corticosteroids in the ICU and reported similar findings, including increased ICU LOS, increased ventilator LOS, increased new onset of infection, and an upward trend in mortality rates.[12] Similarly, Lu et al. conducted a study using data from MIMIC-III (an earlier version of MIMIC-IV) and determined that administering systemic corticosteroids to patients with septic shock resulted in higher 30-day mortality rates among those with metastatic cancer, while it did not improve mortality rates in immunocompromised patients.[7] They also observed that use of systemic corticosteroids was associated with hemodynamic stability, long ICU and hospital LOS and an increased risk of hyperglycemia.[7] Collectively, these results indicate that corticosteroid use in patients with sepsis may result in noteworthy negative consequences and should be employed with careful consideration.
The findings of this research are a valuable addition to the ongoing discourse regarding the mortality implications of utilizing corticosteroids to treat patients with sepsis and septic shock. The two most recent RCTs on corticosteroid treatment for sepsis reported contradictory conclusions on 90-day mortality.[22,23] The ADRENAL trial, which included 3,658 patients with septic shock, found no statistically significant difference between hydrocortisone and placebo in terms of 90-day mortality.[22] In contrast, the APROCCHSS trial, which included 1,241 patients with septic shock, reported that hydrocortisone and fludrocortisone combination reduced 90-day mortality compared to placebo.[23] These trials were included in a linked systematic review with other RCTs comparing corticosteroids with placebo in patients with sepsis and/or septic shock. The BMJ Rapid Panel of Recommendation carefully reviewed and translated the evidence using GRADE methodology for trustworthy guidelines and concluded that while corticosteroids may have a positive effect on mortality, the evidence was considered uncertain due to the inconsistency of results across RCTs.[24,25] Although recent meta-analyses have been conducted, a conclusive consensus has yet to be reached regarding the use of corticosteroids in patients with sepsis or septic shock.[6,24,26-31] Our study examined patients admitted to the ICU with sepsis or septic shock and found that administering corticosteroids was associated with increased ICU mortality rates. However, other investigations have reported no reduction in mortality or LOS in the ICU.[3,10,32]
Corticosteroids are known to have immunosuppressive effects, as documented in previous studies.[33] Severe depression of the immune system due to circulating inflammatory mediators during trauma and infection is also well understood.[34] The combination of these two effects on the immune system could explain the increased onset of new infections and ICU mortality found in our study. Furthermore, all-cause immunosuppression has been associated with an increased risk of mortality.[35-38] Our study found that the mean ICU LOS was prolonged by 2 days in the corticosteroid user group, and a higher percentage of patients in this group required mechanical ventilation (41.7%). These results could be attributed to the secondary effect of the increased infection rate in the corticosteroid group. In addition, hyperglycemia is a well-known adverse effect of corticosteroids,[7] which could explain why the percentage of patients with incident hyperglycemia (5.18%) was higher in the corticosteroid group. Overall, these findings provide important insights into the potential adverse effects of corticosteroids in patients with sepsis and suggest that clinicians should carefully consider their use in this population.
This study has several strengths and limitations. The MIMIC-IV data are the most recent version of the MIMIC database which included large patient population size with updated real-world electronic medical records. As a result, evidence generated is updated evidence among ICU patients and which represents the critical care practice reality within the most recent decade. This study utilized the novel AIPW approach to account for the inherent selection bias resulting from “self-selection” toward treatment with corticosteroids to generate doubly robust estimates which are considered unbiased ATEs of corticosteroids use.[20] Specifically, AIPW approach generates an unbiased ATE of corticosteroid use in terms of 30-day ICU mortality, ICU LOS, new onset of infection, diagnosis of hyperglycemia and use of mechanical ventilation.
While interpreting the results of this study, it is important to consider its limitations. The MIMIC-IV database, which was the source of the data used, is a real-world data collected from a single center, which may limit external validity and generalizability beyond BIDMC centers in Massachusetts. However, as intensivists and other clinicians are expected to be guided by similar clinical practice guidelines, we do not anticipate a significant difference in practice across ICUs in the United States. Nevertheless, the included variables were limited to those available in the data, which may have resulted in unmeasured residual confounding factors. The MIMIC-IV data did not include a date of death variable, only a 30-day mortality variable, which limited our ability to assess mortality for longer periods, such as 60-day or 90-day mortality. Therefore, the study only provides evidence on short-term mortality assessment. Finally, the study utilized data from 2008 to 2019, and treatment guidelines may have changed over time. While it may be helpful to adjust for calendar year in the propensity score model in future studies, this limitation should be considered when interpreting the current findings.
CONCLUSION
This study’s findings highlight that administering systemic corticosteroids, such as dexamethasone, hydrocortisone, and methylprednisolone, to treat sepsis in ICU patients is associated with increased rates of 30-day ICU mortality, ICU LOS, mechanical ventilation use, new onset of infection, and hyperglycemia diagnosis. While there are clinical practice guidelines in place for the use of corticosteroids in sepsis patients, the evidence supporting their use remains weak and uncertain. In light of the findings presented in this study and the current literature, we recommend that clinicians treating sepsis patients in the ICU remain diligent in their decision-making process when prescribing corticosteroids, taking into account all available evidence and patient preferences.
Acknowledgment
The authors sincerely thank the MIT Laboratory for Computational Physiology and collaborating research groups for providing the new MIMIC data -MIMIC-IV version 0.4 and for also providing statistical analysis software programs for calculating SOFA scores and modified Angus abstraction program for sepsis. We also appreciate the National Institute of Biomedical Imaging and Bioengineering of the National Institutes of Health who through the grant awards (R01EB030362) supports to the MIT Laboratory for Computational Physiology and collaborating research groups, MIMIC-IV version 0.4 data were made available.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflict of interest.
Supplementary materials
Result of the sensitivity analysis.
SUPPLEMENTARY TABLE
| Low dose-long course steroid users versus non-steroid users | ||||||||||||||
| Primary outcomes | ||||||||||||||
| 30-Day ICU mortality | ICU length of stay | |||||||||||||
| Estimate | Wald | 95% CL | P | Estimate | Wald | 95% CL | P | |||||||
| Parameter | ||||||||||||||
| POM | Steroids users | 0.305 | 0.221 | 0.388 | <0.0001 | 8.389 | 6.491 | 10.287 | <0.0001 | |||||
| POM | Non-users | 0.130 | 0.116 | 0.144 | <0.0001 | 4.812 | 4.576 | 5.048 | <0.0001 | |||||
| ATE | 0.175 | 0.090 | 0.259 | <0.0001 | 3.577 | 1.666 | 5.488 | 0.0002 | ||||||
| Secondary outcomes | ||||||||||||||
| Mechanical ventilation | New onset of infection | Hyperglycemia | ||||||||||||
| Estimate | Wald 95% CL | P | Estimate | Wald 95% CL | P | Estimate | Wald 95% CL | P | ||||||
| Parameter | ||||||||||||||
| POM | Steroids users | 0.518 | 0.427 | 0.608 | <0.0001 | 0.140 | 0.086 | 0.194 | <0.0001 | 0.046 | 0.027 | 0.066 | <0.0001 | |
| POM | Non-users | 0.287 | 0.269 | 0.305 | <0.0001 | 0.045 | 0.036 | 0.053 | <0.0001 | 0.023 | 0.020 | 0.027 | <0.0001 | |
| ATE | 0.231 | 0.138 | 0.323 | <0.0001 | 0.096 | 0.041 | 0.150 | 0.0006 | 0.023 | 0.003 | 0.043 | 0.0223 | ||
POM: Potential outcome means, ATE: Average treatment effect, CL: Confidence limit, P:P-value. Each model controlled for: Age group, race category, insurance, SOFA score: The sequential organ failure assessment, laboratory tests and vital signs, MECI: Modified Elixhauser comorbidity index, ICU subtypes, statin use, BMI, and data year category. Statistically significant at alpha significant level ≤0.05
Financial support and sponsorship
None.
References
- Prevalence, underlying causes, and preventability of sepsis-associated mortality in US acute care hospitals. JAMA Network Open. 2019;2:e187571.
- [CrossRef] [PubMed] [Google Scholar]
- Sepsis: A roadmap for future research. Lancet infect Dis. 2015;15:581-614.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA. 2002;288:862-871.
- [CrossRef] [PubMed] [Google Scholar]
- New decade, old debate: Blocking the cytokine pathways in infection-induced cytokine cascade. Crit Care Explor. 2021;3:e0364.
- [CrossRef] [PubMed] [Google Scholar]
- Steroids in the treatment of clinical septic shock. Ann Surg. 1976;184:333-341.
- [CrossRef] [PubMed] [Google Scholar]
- Association of corticosteroid treatment with outcomes in adult patients with sepsis: A systematic review and meta-analysis. JAMA Intern Med. 2019;179:213-223.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy and safety of corticosteroids for septic shock in immunocompromised patients: A cohort study from MIMIC. Am J Emerg Med. 2021;42:121-126.
- [CrossRef] [PubMed] [Google Scholar]
- The effects of high-dose corticosteroids in patients with septic shock: A prospective, controlled study. N Engl J Med. 1984;311:1137-1143.
- [CrossRef] [PubMed] [Google Scholar]
- A controlled clinical trial of high-dose methylprednisolone in the treatment of severe sepsis and septic shock. N Engl J Med. 1987;317:653-658.
- [CrossRef] [PubMed] [Google Scholar]
- Hydrocortisone therapy for patients with septic shock. N Engl J Med. 2008;358:111-124.
- [CrossRef] [PubMed] [Google Scholar]
- Corticosteroids in the treatment of severe sepsis and septic shock in adults: A systematic review. JAMA. 2009;301:2362-2375.
- [CrossRef] [PubMed] [Google Scholar]
- Corticosteroid use in the intensive care unit: At what cost? Arch Surg. 2006;141:145-149. discussion 149
- [CrossRef] [PubMed] [Google Scholar]
- Surviving sepsis campaign: International guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43:304-377.
- [CrossRef] [PubMed] [Google Scholar]
- MIMIC-IV (version 0.4) PhysioNet. 2020. Available online: https://physionet.org/content/mimiciv/1.0/ [Last accessed on 2021 Aug 23]
- [Google Scholar]
- Strengthening the reporting of observational studies in epidemiology-nutritional epidemiology (STROBE-nut): An extension of the STROBE statement. Nutr Bull. 2016;41:240-251.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the angus ICD9-CM sepsis abstraction criteria. bioRxiv. 2017;124289
- [CrossRef] [Google Scholar]
- Identifying patients with severe sepsis using administrative claims: Patient-level validation of the angus implementation of the international consensus conference definition of severe sepsis. Med Care. 2014;52:e39-e43.
- [CrossRef] [PubMed] [Google Scholar]
- Concept: Elixhauser Comorbidity Index: University of Manitobap. 2020. Available from: https://www.mchp-appserv.cpe.umanitoba.ca/viewConcept.php?conceptID=1436 [Last accessed on 2021 May 25]
- [Google Scholar]
- The impact of statin use prior to intensive care unit admission on critically ill patients with sepsis. Pharmacotherapy. 2021;41:162-171.
- [CrossRef] [PubMed] [Google Scholar]
- Estimating Causal Effects from Observational Data with the CAUSALTRT Procedure. In: Paper Presented at: Proceedings of the SAS Global Forum 2017 Conference. Cary, NC: SAS Institute Inc; 2017. Available from: https://www.support.sas.com/resources/papers/proceedings17/SAS0374-2017 [Last accessed on 2022 Sep 08]
- [Google Scholar]
- Balance diagnostics after propensity score matching. Ann Transl Med. 2019;7:16.
- [CrossRef] [PubMed] [Google Scholar]
- Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med. 2018;378:797-808.
- [CrossRef] [PubMed] [Google Scholar]
- Hydrocortisone plus fludrocortisone for adults with septic shock. N Engl J Med. 2018;378:809-818.
- [CrossRef] [PubMed] [Google Scholar]
- Corticosteroids in sepsis: An updated systematic review and meta-analysis. Crit Care Med. 2018;46:1411-1420.
- [CrossRef] [PubMed] [Google Scholar]
- Corticosteroid therapy for sepsis: A clinical practice guideline. BMJ. 2018;362:k3284.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of adjunctive corticosteroids on clinical outcomes in adult patients with septic shock-a meta-analysis of randomized controlled trials and trial sequential analysis. J Crit Care. 2018;48:296-306.
- [CrossRef] [PubMed] [Google Scholar]
- Low-dose corticosteroids for adult patients with septic shock: A systematic review with meta-analysis and trial sequential analysis. Intensive Care Med. 2018;44:1003-1016.
- [CrossRef] [PubMed] [Google Scholar]
- Do low-dose corticosteroids improve survival or shock reversal from septic shock in adults? Meta-analysis with trial sequential analysis. J Int Med Res. 2018;46:2513-2524.
- [CrossRef] [PubMed] [Google Scholar]
- Can corticosteroids reduce the mortality of patients with severe sepsis? A systematic review and meta-analysis. Am J Emerg Med. 2019;37:1657-1664.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of low-dose hydrocortisone therapy in adult patients with septic shock: A meta-analysis with trial sequential analysis of randomized controlled trials. J Intensive Care Med. 2020;35:971-983.
- [CrossRef] [PubMed] [Google Scholar]
- Impact and beneficial critical points of clinical outcome in corticosteroid management of adult patients with sepsis: Meta-analysis and grade assessment. Front Pharmacol. 2019;10:1101.
- [CrossRef] [PubMed] [Google Scholar]
- Early initiation of low-dose hydrocortisone treatment for septic shock in adults: A randomized clinical trial. Am J Emerg Med. 2017;35:1810-1814.
- [CrossRef] [PubMed] [Google Scholar]
- Corticosteroids and infectious diseases. Med Clin North Am. 1973;57:1277-1287.
- [CrossRef] [PubMed] [Google Scholar]
- Immune dysfunction in trauma. Surg Clin North Am. 1999;79:1385-1416.
- [CrossRef] [PubMed] [Google Scholar]
- Consequences of high-dose steroid therapy for acute spinal cord injury. J Trauma. 1997;42:279-284.
- [CrossRef] [PubMed] [Google Scholar]
- Septic complications of corticosteroid administration after central nervous system trauma. Ann Surg. 1985;202:248-252.
- [CrossRef] [PubMed] [Google Scholar]
- Time course of septic shock in immunocompromised and nonimmunocompromised patients. Crit Care Med. 2017;45:2031-2039.
- [CrossRef] [PubMed] [Google Scholar]
- Sepsis severe or septic shock: Outcome according to immune status and immunodeficiency profile. Chest. 2014;146:1205-1213.
- [CrossRef] [PubMed] [Google Scholar]




